SciresolSciresolhttps://jmsh.ac.in/Journal of Medical Sciences and Health10.55289/jnutres/v13i2.25.65ORIGINAL ARTICLE<p>Design and Validation of a Context-Specific Nutritional Screening Tool for Clinical Setting</p>303202520251321Abstract
<p>Hospital malnutrition risk is common at admission and linked to poor outcomes. Existing screening tools often require adaptation to suit patient needs and hospital settings. The study aims to assess the knowledge, attitudes, and practices (KAP) about nutritional screening tool usage by healthcare professionals and to develop and evaluate a modified screening tool. A structured questionnaire was developed using google forms and distributed to 50 healthcare professionals. Subsequently, a cross-sectional study was carried out involving 173 cardiac patients aged 30–60 years. KAP insights highlighted the importance of screening and the need to modify tools. Among the 173 patients, 35% were at low nutritional risk, 59% at medium risk, and 7% at high risk. Items with discrimination index scores below 0.2 were removed. The tool demonstrated strong internal consistency (Cronbach’s alpha = 0.70 -- 0.90) and excellent test–retest reliability (r = 0.97), confirming its reliability and robustness. The modified nutritional screening tool was found to be time-efficient, resource-conserving, valid, practical, and suitable for hospital use. Further studies are recommended to apply it across diverse clinical groups.</p>
KeywordsNutrition care processNutrition screening and assessmentNutrition interventionMalnutritionCardiac patientsVermaShivangi12 Research Scholar, Department of Food and Nutritional Sciences Sri Sathya Sai Institute of Higher Learning Anantapur – 515001, Andhra Pradesh India Dietitian, Department of Dietary Sri Sathya Sai Institute of Higher Medical Sciences Puttaparthi, 5151001, Andhra Pradesh India Assistant Professor, Department of Food and Nutritional Sciences Sri Sathya Sai Institute of Higher Learning Anantapur – 515001, Andhra Pradesh IndiaSumanaAraveti3 Research Scholar, Department of Food and Nutritional Sciences Sri Sathya Sai Institute of Higher Learning Anantapur – 515001, Andhra Pradesh India Dietitian, Department of Dietary Sri Sathya Sai Institute of Higher Medical Sciences Puttaparthi, 5151001, Andhra Pradesh India Assistant Professor, Department of Food and Nutritional Sciences Sri Sathya Sai Institute of Higher Learning Anantapur – 515001, Andhra Pradesh India1 Introduction
Hospital-acquired malnutrition affects approximately 65% of inpatients, indicating a significant clinical and public health concern within healthcare settings[1]. The World Health Organization (WHO) defines malnutrition as deficit (undernutrition) or excess of nutrients (overnutrition) that can adversely impact overall health[2]. India is one of the fastest growing countries and second largest urban population globally. According to the WHO, malnutrition is a burden on public health worldwide. In 2022, approximately 2.5 billion adults worldwide were classified as overweight, with 890 million living with obesity and 390 million identified as underweight[2]. India accounts for nearly one-third of the global undernutrition burden. Several government schemes are working towards reducing malnutrition and hunger rates[3].
Malnutrition can result from inadequate intake, increased needs due to illness or surgery, malabsorption, prolonged hospitalization, and inadequate screening or intervention. It may lead to delayed healing, higher infection rates, longer hospital stays (LOS), increased morbidity and mortality, and reduced quality of life[4]. Nutritional screening on admission, results in early identification of malnutrition which leads to mitigate in hospital complications, hasten recovery, shorten LOS, and lower risk for hospital readmission[5].
Widely used nutritional screening tools such as Malnutrition Universal Screening Tool (MUST), Nutrition Risk Status 2002 (NRS 2002), Subjective Global Assessment (SGA) and Mini-Nutritional Assessment (MNA) were designed and developed within western healthcare settings. Existing tools emphasize on individual weight status and underlying disease, which may limit their applicability in certain clinical settings[6]. Due to which, these tools are not meeting the standards of diverse global populations, such as those in India, Africa and Southeast Asia[7]. However, greater emphasis should be placed on the underlying disease etiology, as it plays a critical role in determining a patient’s nutritional status[8].
These well-established tools are mostly unsuitable, due to the differences in cultural, dietary, and socioeconomic factors. However, these tools lack specificity in various medical diagnosis or disease conditions such as patients with cardiac disease[9], renal, or oncological conditions and patients who are in need of specific nutritional support[10]. Furthermore, the usage and applicability of these tools differ from the type of healthcare setting. Most importantly it depends upon different hospital resources available and patient profiles compared to primary or rural healthcare facilities. Hence, there is a need for context-specific, validated nutritional screening tools that are designed and developed according to the local cultural factors, dietary habits and practices, disease patterns, and healthcare infrastructure. Efficient identification of patients resulting in targeted nutritional interventions occurs when screened immediately upon hospital admission, using tools that are convenient, rapid (requiring less than five minutes), and non-invasive[11].
The use of simple, quick screening and assessment tools enables healthcare professionals preferably dietitians to promptly identify individuals at risk of malnutrition[12, 13]. A thorough assessment should integrate subjective inputs such as clinical history and physical examination, along with objective measures including body composition, functional assessments, and laboratory values to accurately evaluate nutritional status. Globally, early identification of malnutrition in hospitals is critical, yet existing screening tools often require adaptation to suit local needs. In India, the Indian Association of Parenteral and Enteral Nutrition (IAPEN) has emphasized the need for a context-specific, simplified screening tool[14].
Therefore, the present study aims to conduct an online KAP survey among health care professionals to elicit information on nutritional screening tools, and to develop and evaluate a modified nutritional screening tool for a hospital setting in India.
2 Methodology
2.1 An online survey to elicit information on knowledge, attitudes and practices associated with nutritional screening and assessment
An online survey was conducted to gather information from healthcare professionals using a structured and pretested questionnaire. The questionnaire was distributed via Google Forms to 50 professionals, including dietitians and registered dietitians, of whom 34 responded. This was conducted in order to gain overall understanding the need of modifying the nutrition screening tools[15]. The survey aimed to assess respondents’ knowledge, attitudes, and practices related to nutritional screening and assessment tools.
The questionnaire comprised twenty logically sequenced questions organized into three sections. The first section collected general demographic and professional information, including name, gender, age, email ID, nature of work, and place of employment. The second section assessed awareness and understanding of nutritional screening and assessment, including definitions, familiarity with existing tools, and preferences for specific instruments. It also explored whether healthcare professionals in their respective institutions modify existing screening tools and, if so, whether these tools have undergone validation. The third section focused on identifying specific parameters that professionals consider both easy to assess and important for nutritional screening and assessment.
2.2 Development of a modified nutritional screening tool
A hospital-based cross-sectional study was conducted at a tertiary care hospital with a capacity of 300 beds. Patient recruitment was carried out using a purposive sampling method from the hospital’s daily admission list. Nutritional screening was performed within 24 to 48 hours of admission. A total of 173 patients were included in the study, based on the inclusion and exclusion criteria, meeting the minimum required sample size to achieve 95% confidence with ±5% precision for the hospital’s patient population.
Data Collection
Anthropometric, biochemical, and clinical data were obtained from patients’ electronic medical records, physical case files, and observations recorded during dietitian-led ward rounds. Nutritional screening was conducted by a registered dietitian through direct patient interaction and clinical observation.
Inclusion Criteria:
Cardiac patients, including those from cardiology and cardiothoracic vascular surgery departments
Age range: 30 to 60 years
Both male and female patients
Patients accompanied by an attender, to ensure reliability of collected data
Exclusion Criteria
Emergency admissions
Pregnant and lactating women
Unstable or critically ill patients
Variable Selection
The variables for the screening tool were guided by a comprehensive review of existing literature, findings from published surveys, and validated tools such as the Malnutrition Universal Screening Tool (MUST) and Nutritional Risk Screening 2002 (NRS2002)[16].
Components of the Screening Tool
The screening tool comprised of ten selected variables: body mass index (BMI), unintentional weight loss, consumption of smoking, alcohol, and tobacco, family history of cardiac disease, dietary habits (including intake of high-fat foods and non-vegetarian diet), clinical symptoms, abnormal vital signs, presence of comorbidities, significant changes in laboratory values, history of surgery (performed or planned), and recommendations for enteral or parenteral nutrition. Recommendations from the Indian Association for Parenteral and Enteral Nutrition (IAPEN), particularly regarding the inclusion of diagnostic components such as physical examination and laboratory assessments within nutritional screening protocols, were also integrated[14].
2.3 Reliability and Validity of the Screening Tool
The consistency and effectiveness of the tool were evaluated through the discrimination index (DI). The DI was calculated to evaluate each item’s ability to differentiate between patients with high and low nutritional risk. Items with DI values below 0.2 were deemed to have poor discriminatory power and were subsequently excluded to enhance the tool’s overall performance.
Reliability was assessed through internal consistency and test–retest methods. Internal consistency was measured using Cronbach’s alpha, to determine the extent to which the components of the tool collectively measured a single underlying construct, with values above 0.7 indicating acceptable reliability.
Test–retest reliability was conducted to examine the tool’s stability and reproducibility over time. The initial screening was performed by the primary investigator on consenting patients, followed by a second assessment by an independent healthcare professional (dietitian) within 2 to 3 days. Both assessors were blinded to each other’s evaluations to minimize bias. Nutritional screening data from both assessments were recorded and compared to evaluate the tool’s temporal reliability.
2.4 Statistical Analysis
Demographic data are presented as means ± standard deviations, while admission characteristics and categorical variables are expressed as percentages. The item discrimination index (DI) and Cronbach’s alpha were calculated to assess reliability and internal consistency. Pearson’s correlation coefficient (r) was employed to evaluate the tool’s validity.
2.5 Ethical Approval
The study was approved by the Institutional Ethics Committee (IEC) of Sri Sathya Sai Institute of Higher Learning, Anantapur (Reg. No. ECR/616/Inst/AP/2014/RR-22). Permission to conduct the study at Sri Sathya Sai Institute of Higher Medical Sciences, Puttaparthi, was granted under reference number SSSIHMS-PG/HR/21/196.
3 Results and Discussions
3.1 An online survey on knowledge, attitudes and practices associated with nutritional screening and assessment
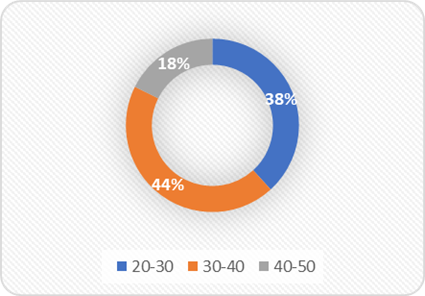
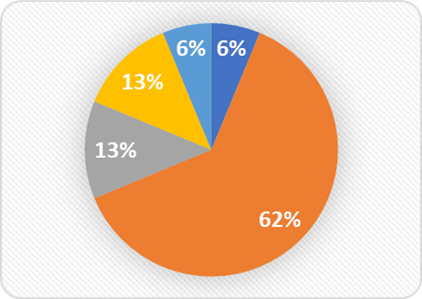
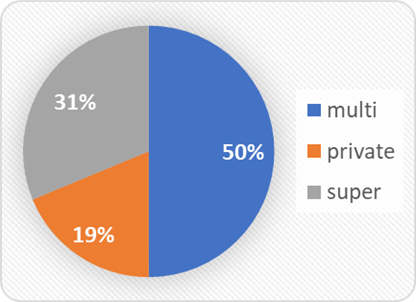
The results of the respondent's survey conducted on a total of 50 respondents were categorized into three age groups. The majority (44%) of healthcare professionals were aged between 30–40 years, 38% in the 20–30 years age category and 18% belonging to the 40–50 years age group [Fig. 1].Survey respondents comprised 68% clinicians and dietitians, 13% interns, 13% registered dietitians, and 6% student interns [Fig. 2]. Among the respondents, 50% were employed in multispecialty hospitals, while 31% worked in super-specialty hospitals. A smaller proportion, 19%, were associated with private clinics or centers [Fig. 3]. This distribution suggests that the majority of respondents were affiliated with large, structured healthcare institutions, which may influence their familiarity with formal nutritional screening practices and protocols[15].
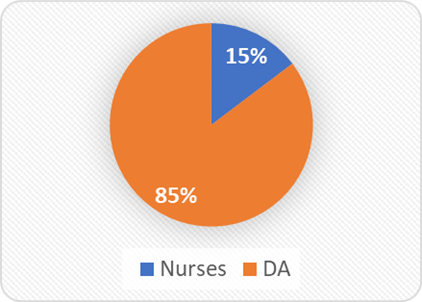
Screening practices of respondents revealed, 85% predominantly comprising dietitians and dietary assistants, screened the patients routinely. However, limited involvement of nursing staff (15%) reflects a missed opportunity for interprofessional collaboration. Given that early detection often occurs during nursing assessments, cross-training programs[17] could enhance screening efficacy and coverage[16]. This distribution highlights that most responses were obtained from dietitians and clinicians, ensuring relevant and informed insights into the use and perception of nutritional screening tools [Fig. 4].
From the survey, 87% of the respondents were aware of the usage and the need for a nutritional screening tool, and 13% of respondents strongly believed that nutritional screening leads to suitable nutritional intervention. The majority of respondents (93%), believed nutritional screening is an important step after admission and before discharge. The survey revealed that 100% of the respondents were aware of at least one nutritional screening and assessment tool. This indicates a high level of general awareness among the respondents regarding the importance and existence of such tools in clinical or nutritional practice.
Fig. 1: Age groups of the respondents
Fig. 2: Nature of work of the respondents
Fig. 3: Work set up of the respondents
Fig. 4: Nutrition screening by respondents
Based on the survey, 20% were unsure about the usage and application of screening tools, MUST, (anthropometry, biochemical, clinical) ABC, SGA, Global Leadership Initiative on malnutrition (GLIM), MNA, Pediatric Nutrition Screening Tool (PNST), NRS2002, and Short Nutritional Assessment Questionnaire (SNAQ) were the most preferred tools across different hospital setups. Modified screening tools were being used by 35% of respondents, while 15% performed screenings manually based on height and weight. Validity and reliability of screening tools was reported by 67% and 13% reported the lack of validity in the tools used.
Consistent with prior research emphasizing early screening upon admission as essential for timely and adequate nutritional care, a recent multi-center study also recommended optimizing dietitian-to-patient ratios and adopted simple, rapid first-line screening tools tailored for Indian healthcare settings[18]. Open-ended suggestions were solicited regarding the items necessary for effective nutritional screening. Respondents' suggestions included the GLIM criteria, causes of weight loss or gain, nutritional knowledge and education, albumin levels, ideal body weight, and electronic health records as items necessary for nutritional screening.
Awareness of validated tools such as MUST (83%), SGA (50%), and NRS-2002 (60%) was moderate, and respondents demonstrated a solid foundational knowledge [Table. 1]. Their knowledge extended to the validity, reliability, and comprehension of these tools, suggesting exposure to and experience with these instruments in clinical settings. However, a notable gap was observed between the recognition of clinical indicators and the perceived ease of measurement for the tools MUST (47%), SGA (40%), and NRS-2002 (40%). This mirrors global findings that while professionals understand the components of malnutrition, operationalizing them remains a challenge due to time constraints, subjective assessments, or lack of training[19].
Popular screening tools
Aware (Yes/No) (%)
Validity(%)
Easy and convenient(%)
MUST
80
60
47
NRS 2002
60
47
40
SGA
53
47
40
Table 1: Knowledge of subjects on existing nutritional screening tools
Therefore, it is important to emphasize the use of nutrition screening and assessment tools at both admission and discharge to address malnutrition and reduce adverse health outcomes among hospitalized patients. Similarly, a study by Zang et al. (2023)[20] used modified nutrition scores to assess nutritional status and effectively measure clinical health outcomes in COVID-19 patients. The results indicated that many clinicians are adapting existing tools to suit the specific needs of their hospital settings and patient populations. For example, Bellanti et al. (2020)[21] aimed to modify screening and assessment tools to better evaluate the presence of sarcopenia. In line with these findings, the present study supports the modification of screening and assessment tools to enhance their relevance, usability, and effectiveness in clinical practice.
3.2 Development of modified nutritional screening tool
Based on insights from the KAP study and extensive literature review, a tool comprising 10 items was developed and evaluated. The characteristics of patients recruited for this study are shown in [Table. 2]. The patients were selected based on the inclusion and exclusion characteristics. The prevalence of malnutrition among cardiac patients is limited[5, 22]. Studies highly recommend screening of cardiac patients on admission[23]. A total of 173 (70% cardiology;29% CTVS) patients (Men: Women-64:36, aged 47.76 ± 9.63 years) were assessed in developing and evaluating the modified nutritional screening tool.
On admission, based on body mass index (BMI), the study found 36% of the patients are undernourished, 48% of patients have normal BMI and 16% patients were overnourished. [Table. 2] shows that study sample consisted of 70% of cardiology patients and 30% of cardiovascular thoracic patients (CTVS) present with comorbidities such as diabetes (19%), hypertension (7%), renal (3%), diabetes and hypertension (18%)[24].
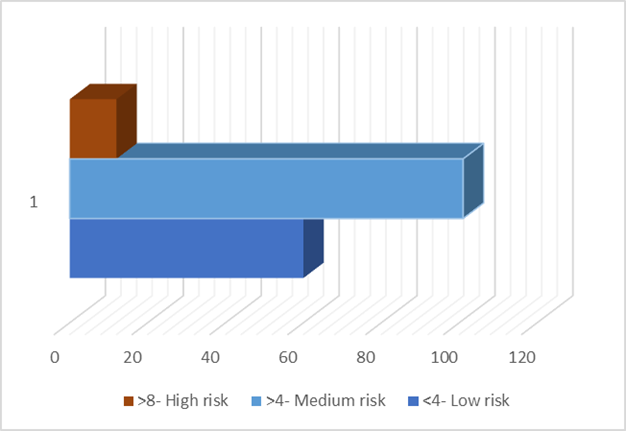
A modified nutritional screening tool revealed 35% of the patient population on admission were at low risk, 59 % were at medium risk and 7 % were at high risk of malnutrition [Fig. 5].
Numerous modified nutritional screening tools have been developed to address specific population needs based on disease type, age group, and hospital setting. For effective clinical use, these tools must be simple, quick, and validated for their target population. The IAPEN through the Chennai Declaration, emphasized the need for a context-specific, streamlined nutritional screening tool suitable for Indian healthcare settings[14].
Variable
Value (Mean ± SD or %)
Age (years)
47.76 ± 9.63
Gender (M: F)
64:36
Height (cm)
158.62 ± 14.48
Weight (kg)
60.34 ± 13.36
BMI (kg/m²)
23.69 ± 4.09
Unintentional weight loss
0.13 ± 0.34
Smoking/alcohol/tobacco use
0.25 ± 0.46
Cardiac family history
0.22 ± 0.42
Non-vegetarian consumption
0.77 ± 0.42
Clinical symptoms
0.75 ± 0.55
Comorbidity (overall)
0.64 ± 0.78
Comorbidity details:
– Diabetes
19%
– Hypertension
7%
– Renal
3%
– Diabetes + Hypertension
18%
Insignificant lab values
1.12 ± 0.80
Surgery performed or planned
0.39 ± 0.61
Enteral/parenteral nutrition recommended
0.01 ± 0.15
Admission type:
– Cardiology
70%
– Cardiothoracic and Vascular Surgery (CTVS)
30%
Table 2: Patient Characteristics and Admission Details (n = 173)
*Values are presented as Mean ± Standard Deviation (SD) for continuous variables and percentages for categorical data.
Comparative evidence from non-cardiac populations supports this approach. For instance, the modified Patient-Generated Subjective Global Assessment (mPG-SGA) was developed and validated specifically for cancer patients, demonstrating improved accuracy in assessing their unique nutritional risks[15]. Similarly, the modified NUTRIC (mNUTRIC) score has been shown to independently predict nutritional risk among patients admitted to surgical intensive care units, aiding in early intervention and improved outcomes[25]. These examples highlight the importance of tailoring nutritional tools to specific clinical populations, reinforcing the rationale for modifying and validating a screening tool specifically for cardiac patients in Indian hospitals, resonating with the present study.
3.3 Reliability and validity of a modified nutritional screening tool
Discrimination index (DI) and Cronbach’s alpha were estimated to assess the consistency of the modified tool and to select appropriate items for the modified tool. [Table. 3] showed that out of the 10 items, 2 items scored DI below 0.2, however, they were retained due to their theoretical importance.
Test-retest validity was investigated in 173 patients. The means of both tests were quite close. There is high correlation (Pearson correlation: 0.9768) between the two tests (close to 1). The p-value is 0.0585, which is slightly above 0.05. The mean scores ranged from 0.01 ± 0.15 for enteral/parenteral nutrition recommendation to 1.12 ± 0.81 for insignificant lab values. DI values indicated moderate to high item discrimination, with comorbidity (DI = 1.02) and insignificant lab values (DI = 0.91) showing the highest discriminative power. The item on unintentional weight loss had the lowest DI (0.14), indicating limited contribution to the overall scale differentiation.
Cronbach’s alpha if item deleted ranged from 0.74 to 0.99, suggesting that the removal of most items would not significantly improve internal consistency. Notably, unintentional weight loss and enteral/parenteral nutrition had the highest alpha values if deleted (0.96 and 0.99 respectively), suggesting weaker internal consistency contributions. Overall, the internal consistency of the tool remained acceptable, with most items supporting scale reliability.
Although the p-value for some items was slightly above 0.05, indicating marginal non-significance, this suggests a potential but inconclusive association with the overall reliability of the tool. These items may not strongly impact internal consistency but should be carefully interpreted rather than immediately excluded. Given the overall acceptable Cronbach’s alpha, the tool remains reliable, though future studies with larger samples may clarify the contribution of such borderline items.
Nutritional screening tool items
Mean Score ± Standard Deviation
Discrimination Index (DI)
Cronbach’s alpha if item deleted
Body mass index
0.70±0.72
0.4
0.74
Unintentional weight loss
0.13±0.34
0.14
0.96
Smoking, alcohol, tobacco
0.25±0.46
0.36
0.93
Cardiac family history
0.21±0.41
0.27
0.94
Non veg consumption
0.77±0.42
0.23
0.95
Clinical symptoms
0.75±0.55
0.38
0.91
Comorbidity
0.63±0.78
1.02
0.8
Insignificant lab values
1.12±0.81
0.91
0.79
Surgeries performed or planned
0.32±0.48
0.27
0.94
Enteral/parenteral nutrition
0.01±0.15
0.04
0.99
Table 3: Internal consistency of the modified nutritional screening tool (n=173)
*Values are presented as Mean ± Standard Deviation (SD). DI refers to the Discrimination Index, indicating the ability of each item to differentiate between groups. Positive DI values suggest good discrimination, while negative values indicate poor or inverse discrimination.
Numerous studies have highlighted the importance of tailoring nutritional screening tools to specific population needs, including disease conditions, age groups, and healthcare settings[26]. A consistent recommendation across the literature is that effective tools must be easy to use, practical for routine clinical workflows, and validated for the target population.
4 Conclusion
The modified nutritional screening tool was successfully developed and validated, demonstrating strong reliability, construct validity, and excellent test–retest consistency (r = 0.97), confirming its effectiveness in accurately identifying malnutrition risk at hospital admission. Its time-efficient, non-invasive, and resource-conserving design makes it highly suitable for routine clinical application in busy hospital environments. When implemented among cardiac patients, the tool not only facilitates early detection of nutritional risk but also helps in planning timely, individualized nutritional interventions and helps in clinical decision-making.
The tool’s validation included internal consistency analysis (Cronbach’s alpha = 0.70–0.90) and discrimination index testing, which led to the refinement of items and strengthened its psychometric robustness. However, a key limitation was the potential for response bias, where patients may have provided socially desirable or inaccurate answers. Future studies should aim on refining or replacing bias-prone items through iterative pilot testing to enhance the tool’s accuracy and reduce the risk of socially desirable responses.
Future studies should focus on multicentric validation of the modified nutritional screening tool across diverse hospital settings to enhance generalizability. Additionally, the tool should be tested in patients with other disease conditions beyond cardiology to evaluate its applicability and predictive accuracy in broader clinical contexts. Incorporating larger and more diverse samples will also strengthen the tool’s reliability and validity.
This study marks a significant advancement in context-specific nutrition screening practices and underscores the tool’s relevance in improving malnutrition detection in Indian hospitals. Future efforts should aim at integrating the tool into national hospital protocols, with potential adaptation as a scalable and efficient nutritional screening model for broader implementation in global healthcare systems.
5 Disclosure
Acknowledgement: The authors from Sri Sathya Sai Institute of Higher Learning (SSSIHL) and Sri Sathya Sai Institute of Higher Medical Sciences (SSSIHMS) dedicated this work to Bhagwan Sri Sathya Sai Baba. The first author would like to express my sincere gratitude to SSSIHL for providing the opportunity to conduct this research and is also grateful to SSSIHMS for the ambience to conduct the study.
Data Availability Statement: The manuscript incorporates all datasets produced or examined throughout this research study
Ethical approval: The study was ethically approved by the Institutional Ethics Committee [IEC] of Sri Sathya Sai Institute of Higher Learning, Anantapur, Sathya Sai district, Anantapur (Reg no. ECR/616/Inst/AP/2014/RR-22. The study also received permission from the Sri Sathya Sai Institute of Higher Medical Sciences, Puttaparthi, Sathya Sai district, Hospital Ethics Committee (Ref no. SSSIHMS-PG/HR/21/196).
Consent to participate: Informed consent was obtained from all individual patients included in the study. Patients were briefed about the purpose, procedures, potential risks, and benefits of the study, and were assured of the confidentiality and voluntary nature of their participation. They were given the right to withdraw at any time without any consequences.
Consent for publication: I hereby consent to the publication of my data and findings, in accordance with the terms outlined by the research team.
Author contribution: Conceptualization & Methodology: Shivangi Verma, Araveti Sumana; Formal Analysis & Data Validation: Shivangi Verma, Araveti Sumana; Experiments & Data Collection: Shivangi Verma;Manuscript Drafting: Shivangi Verma; Manuscript Review & Editing: Araveti Sumana; Supervision: Araveti Sumana; Final Approval: All authors read and approved the final manuscript.
References
Cass AR, Charlton KE
Prevalence of hospital‐acquired malnutrition and modifiable determinants of nutritional deterioration during inpatient admissions: A systematic review of the evidenceJournal of Human Nutrition and Dietetics2022356https://doi.org/10.1111/jhn.13009
Nakyeyune R, Ruan XL, Shen Y, Shao Y, Niu C, Zang ZP, <I>et al</I>
Diagnostic Accuracy of the Malnutrition Screening Tool (MST) in Adult Cancer Patients: A Systematic Literature Review and Meta-AnalysisJournal of Nutritional Oncology202161https://doi.org/10.34175/jno202101003
van Vliet IMY, Gomes-Neto AW, de Jong MFC, Jager-Wittenaar H, Navis GJ
High prevalence of malnutrition both on hospital admission and predischargeNutrition202077https://doi.org/10.1016/j.nut.2020.110814
Correia MITD, Sulo S, Brunton C, Sulz I, Rodriguez D, Gomez G, <I>et al</I>
Prevalence of malnutrition risk and its association with mortality: nutritionDay Latin America survey resultsClinical Nutrition2021409https://doi.org/10.1016/j.clnu.2021.07.023
Hiura G, Lebwohl B, Seres DS
Malnutrition Diagnosis in Critically Ill Patients Using 2012 Academy of Nutrition and DieteticsJournal of Parenteral and Enteral Nutrition2020442https://doi.org/10.1002/jpen.1599
Inciong JFB, Chaudhary A, Hsu HS, Joshi R, Seo JM, Trung LV, <I>et al</I>
Hospital malnutrition in northeast and southeast Asia: A systematic literature reviewClinical Nutrition ESPEN202039https://doi.org/10.1016/j.clnesp.2020.06.001
Rattanachaiwong S, Zribi B, Kagan I, Theilla M, Heching M, Singer P
Comparison of nutritional screening and diagnostic tools in diagnosis of severe malnutrition in critically ill patientsClinical Nutrition20203911https://doi.org/10.1016/j.clnu.2020.02.035
Chen XY, Zhang XZ, Ma BW, Li B, Zhou DL, Liu ZC, <I>et al</I>
A comparison of four common malnutrition risk screening tools for detecting cachexia in patients with curable gastric cancerNutrition202070https://doi.org/10.1016/j.nut.2019.04.009
Chávez-Tostado M, CervaChávez-Tostado M, Cervantes-Guevara G, López-Alvarado SE, Cervantes-Pérez G, Barbosa-Camacho FJ, Fuentes-Orozco C, <I>et al</I>ntes-Guevara G, López-Alvarado SE, Cervantes-Pérez G, Barbosa-Camacho FJ, Fuentes-Orozco C, <I>et al</I>
Comparison of nutritional screening tools to assess nutritional risk and predict clinical outcomes in Mexican patients with digestive diseasesBMC Gastroenterology2020201https://doi.org/10.1186/s12876-020-01214-1
Bramley A, Forsyth A, McKenna L
Validity and Educational Impact of Clinical Entrustable Professional Activities Linked to the Nutrition Care Process for Work-Based Assessment of Entry-Level Dietetics Students: Evaluation of a 3-Year Implementation Study in AustraliaJournal of the Academy of Nutrition and Dietetics20231234https://doi.org/10.1016/j.jand.2022.09.009
Reber E, Gomes F, Vasiloglou MF, Schuetz P, Stanga Z
Nutritional Risk Screening and AssessmentJournal of Clinical Medicine201987https://doi.org/10.3390/jcm8071065
Krznarić Ž, Bender DV, Laviano A, Cuerda C, Landi F, Monteiro R, <I>et al</I>
A simple remote nutritional screening tool and practical guidance for nutritional care in primary practice during the COVID-19 pandemicClinical Nutrition2020397https://doi.org/10.1016/j.clnu.2020.05.006
Timmanpyati S, Varma S, Pottakkat B, Vijayakumar PC, Sreedharan L, Patel D, <I>et al</I>
The IAPEN INDIA Association for Parenteral and Enteral Nutrition Chennai Declaration on the Fundamental Right to Nutritional Care of Patients Under TreatmentJournal of Nutrition Research2023111https://doi.org/10.55289/jnutres/v11i1_22.27
Fu Z, Zhang R, Wang KH, Cong MH, Li T, Weng M, <I>et al</I>
Development and validation of a Modified Patient‐Generated Subjective Global Assessment as a nutritional assessment tool in cancer patientsJournal of Cachexia, Sarcopenia and Muscle2022131https://doi.org/10.1002/jcsm.12872
Serón-Arbeloa C, Labarta-Monzón L, Puzo-Foncillas J, Mallor-Bonet T, Lafita-López A, Bueno-Vidales N, <I>et al</I>
Malnutrition Screening and AssessmentNutrients20221412https://doi.org/10.3390/nu14122392
Varma S, Kapoor M, Patil M, Patel D, Timmanpyati S
Survey of Nutritional Screening Status as Well as Dietitian to Patient Ratio in Various Healthcare Setups in IndiaJournal of Nutrition Research2023111https://doi.org/10.55289/jnutres/v11i1_22.24
Cederholm T, Jensen GL, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, <I>et al</I>
GLIM criteria for the diagnosis of malnutrition – A consensus report from the global clinical nutrition communityClinical Nutrition2019381https://doi.org/10.1016/j.clnu.2018.08.002
Zang Y, Xu W, Qiu Y, Gong D, Fan Y
Association between Risk of Malnutrition Defined by the Nutritional Risk Screening 2002 and Postoperative Complications and Overall Survival in Patients with Cancer: A Meta-AnalysisNutrition and Cancer2023758https://doi.org/10.1080/01635581.2023.2227402
Bellanti F, Lo Buglio A, Quiete S, Pellegrino G, Dobrakowski M, Kasperczyk A, <I>et al</I>
Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older PatientsJournal of Clinical Medicine202096https://doi.org/10.3390/jcm9061898
Pathirana AK, Lokunarangoda N, Ranathunga I, Santharaj WS, Ekanayake R, <I>et al</I>
Prevalence of hospital malnutrition among cardiac patients: Results from six nutrition screening toolsSpringerPlus201431https://doi.org/10.1186/2193-1801-3-412
Vadiveloo M, Lichtenstein AH, Anderson C, Aspry K, Foraker R, Griggs S, <I>et al</I>
Rapid Diet Assessment Screening Tools for Cardiovascular Disease Risk Reduction Across Healthcare Settings: A Scientific Statement From the American Heart AssociationCirculation: Cardiovascular Quality and Outcomes2020139https://doi.org/10.1161/hcq.0000000000000094
Cuong TQ, Banks M, Hannan-Jones M, Thi Ngoc Diep D, Gallegos D
Validity, reliability and feasibility of nutrition screening tools NRS-2002 and MST administered by trained medical doctors in routine practiceHospital Practice2019475https://doi.org/10.1080/21548331.2019.1699760
Zhang P, He Z, Yu G, Peng D, Feng Y, Ling J, <I>et al</I>
The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patientsClinical Nutrition2021402https://doi.org/10.1016/j.clnu.2020.05.051
Atef H, Abdel-Raouf R, Zeid AS, Elsebaie EH, Abdalaleem S, Amin AA, <I>et al</I>
Development of a simple and valid nutrition screening tool for pediatric hospitalized patients with acute illnessF1000Research202110https://doi.org/10.12688/f1000research.51186.1